ACNE is an inflammatory skin condition, commonly affecting the face, chest and back. It is one of the most common skin conditions, affecting up to 80-90% of adolescents. Acne may also occur during infancy due to the activation of sebaceous glands by maternal hormones in-utero. It can be a persistent problem, although it spontaneously resolves after a period of 4-5 years in about 70% of people. Approximately 30% of people continue with their acne into adult life. The incidence of acne at the age of 40 is reported to be 1% in men and 5% in women. Causes
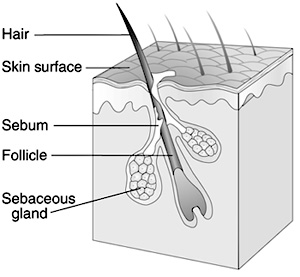
Acne is caused by the overactivity of the sebaceous (oil) glands. Sebaceous glands are active due to the hormone testosterone. Testosterone is produced in men from the testes and in women from the ovaries and the adrenal gland. Although testosterone levels are usually normal in people who develop acne, the sebaceous glands are overly sensitive to the hormone. Over production of oil leads to a greasy feel to the skin. In addition, there is a change in the growth of the cells lining the follicular canal (pore). Instead of dislodging normally and being carried away by the oil (sebum) when they die, these cells become sticky and stick to the inner surface of the gland and gradually build up a partial blockage.
Symptoms
The partial blockage of the pore is called a microcomedone and is the precursor of all inflammatory and non-inflammatory spots in acne. Bacteria start to multiply within the blockage, which leads to inflammatory lesions or red papules. As part of the healing process, the body recruits white blood cells which destroy the bacteria but lead to the formation of pus, leading to comedones (blackheads), small pimples, large pustules, or painful swollen cysts. There are many myths surrounding the causes of acne, which include:
- only teenage spots - you'll grow out of it.
- eating too much chocolate and too
many chips.
- not keeping your skin clean enough.
Acne can be a devastating psychological disease commonly affecting the face, neck, chest, shoulders and back. The latest survey by the Acne Support Group shows that 12% of people with acne feel suicidal as a result of having the condition. Whilst it is a very common skin condition, it need not be left untreated and leave a person feeling so desperate that they want to take their own life.
Treatments
There are many treatments available, which need to be given at an early stage to prevent scarring. Treatments are generally longterm, however with encouragement and support a person can improve their skin substantially.
First line treatment for acne includes creams or gels containing the active ingredient benzoyl peroxide, which is available from chemists. Salicylic acid is also available from chemist shops and can be effective in comedonal (blackhead) type acne. Antibiotics are a very popular treatment for acne. These help to reduce inflammation, whilst
killing the bacteria. Other treatments include preparations containing the hormone therapy cyproterone acetate (females only).
For those who have not responded to
systemic and topical therapies, isotretinoin, which is a synthetic vitamin A, can be very useful. This is a hospital-only drug and can achieve up to 95% positive results in patients. There are many potential side effects from this drug and hence the patient
will need monitoring by their dermatologist.
Generally, treatments need to be taken
for two months before any improvement is noticed
ALOPECIA
Alopecia is a generic medical term for all forms of hair loss, from the patchy baldness of alopecia areata, which in some cases becomes total loss, to the diffuse thinning and alopecia androgenetica. Hair loss can be sudden, frightening and severe. Although it is not life threatening or even physically painful, alopecia causes a high level of psychological and emotional suffering. A survey by Hairline International of women who had lost, or were losing, their hair found that 76% felt less of a woman; 40% said that marriages (or long term partnerships) had suffered and of these many had broken up; and 63% said they had been forced to compromise a career. In many cases, alopecia patients experience severe depression. A large proportion of the respondents (43%) had considered suicide. In addition, patients often face cruel jokes from others and find that some healthprofessionals dismiss the condition as superficial.
Types and Symptoms
Alopecia areata (patchy baldness) affects men, women and children. It often begins at puberty. This scalp disease usually starts with a tiny circumscribed patch of baldness. Other patches may follow and as one patch re-grows hair frequently falls out in another. Alopecia areata frequently spreads very quickly, sometimes throughout the scalp. The affected hair follicles slow down production, become very small and often grow no hair that is visible above the surface for months or years. But the follicles normally remain alive and are ready to resume normal hair production whenever they receive the appropriate signal. In a third of all cases patients will have only one small patch of baldness. The hair re-grows spontaneously and they never suffer a further episode. Two thirds of patients suffer the patchy baldness of alopecia areata throughout their lives.
Alopecia areata can develop into total loss of scalp hair (alopecia totalis) or the loss of all body hair including the scalp - alopecia universalis - which occurs in about one fifth of cases.
Alopecia androgenetica (male pattern baldness) - a large number of women suffer from thinning hair. In a woman this can be the female version of alopecia androgenetica, the natural balding of ageing. It often occurs after the menopause, but is also prevalent in younger women who are genetically predisposed to the condition. It can manifest itself when triggered by such factors as eating disorders or an over-sensitivity to the progestogens contained in some types of contraceptive pill.
Male pattern baldness often causes a great deal of distress, particularly in men whose work brings them into contact with the public. It can cause a marked fall in self-esteem.
Telogen effluvium - lass occurs after the body has suffered severe trauma. It can occur after a high fever, childbirth or extreme shock.
Hair loss related to medication -Some drugs prescribed for other conditions can cause hair thinning. Including some psychiatric drugs (eg. anti-depressants) and chemotherapy treatment.
Self-inflicted hair loss -Trichotillomania is an obsessional compulsive disorder in which many patients pull out their own hair.
Causes
Alopecia areata is believed to be an autoimmune disease in which the body rejects the hair follicle as foreign. Atopic syndrome often plays a part and alopecia areata frequently occurs in patients who have experienced asthma or eczema from birth. Other factors, which can be involved in its onset, are thyroid conditions, anaemia, vaccinations and stress. It can also be a family problem. One in five patients can recall a relative with a similar condition.
Many younger women develop alopecia androgenetica, because they have an over-sensitivity to the androgens (male hormones) in the blood. When they have this pre-disposed sensitivity, contraceptive pills containing progestogen can exacerbate the problem. Hormone replacement therapy (HRT) has similar components to the pill and many women find that their hair becomes thinner during this treatment. The stress of modern life is a common causative agent.
Treatments
Re-growth success is not always easy to achieve and doctors are cautious of raising false hope by offering treatment. For alopecia areata, and its related conditions, re-growth success has been achieved by the use of a combination therapy consisting of topical steroid creams plus topical minoxidil, systemic steroids (such as prednisolone) and, occasionally, zinc. The administration of powerful steroids can sometimes be enough to 'kick-start' the hair into re-growth, although doctors urge caution and careful monitoring for side-effects. In severe cases and those of total loss, the phenol derivative diphencyprone can be successful. In less severe cases of both Alopecia Androgenetica and Alopecia Areata, topical minoxidil alone can promote re-growth. Anti-androgen drugs such as cyproterone acetate can also help in alopecia androgenetica. Finasteride, the drug for the treatment of enlarged male prostate, has recently been licensed for the treatment of hair loss in men.
BULLOUS PEMPHIGOID
Bullous pemphigoid is a rare, blistering skin disease which can occur anywhere on the skin, but is more commonly found on the folds of the skin, particularly the groin area and the armpits. The disease is more prevalent in the elderly, but an increasing number of people are being diagnosed when in their early fifties. The average age of onset for the disease is between 65 and 75. The condition affects males and females in equal proportion and is rarely life-threatening. In approximately 30% of people the condition burns itself out after a number of years, although a recurrence can occur in later life.
Causes
Bullous pemphigoid is an autoimmune disease, where an immune response is triggered to the skin cells. Separation occurs between the epithelial and dermal layers of the skin. The reason for this immune response remains the subject of research. The condition is not contagious and may not be passed on by skin contact.
Symptoms
During a flare-up a non-specific rash first develops on the folds of the limbs. The skin becomes inflamed (erythematous) and very itchy (pruritic). The patient reports feeling very tired and agitated. The disease is at times very debilitating and distressing, with simple tasks becoming a real effort to perform. The stress of the disease can exacerbate the condition. These changes can resemble other skin diseases, such as urticaria, erythema multiforme and dermatitis herpetiformis. Consequently GPs often do not recognise these signs as the early symptoms of bullous pemphigoid. Following this (prodromal) phase, fluid-filled blisters develop. A diagnosis of the condition is confirmed by examination of a blister by skin biopsy. The prodromal phase can last from a single week to several months. Although the condition sometimes remains localised, it is more common for dense bullae to progressively cover both inflamed and normal skin over the majority of the body area. The skin feels hot, itchy and very tender. The lesions, which can be several centimetres in diameter, are particularly concentrated in body folds. Lesions may also develop in the mouth and other mucosal membranes.
Treatments
When a widespread blistering flare-up occurs, the patient is usually admitted to hospital. As yet there is no cure for bullous pemphigoid, but the condition can be controlled using potent medications. Depending on the severity of the blistering and the general health, it can be treated very successfully using steroids and/or immunosuppressants. A large initial dosage of steroids is administered during a flare-up, in order to bring the blistering under control. These treatments can have harmful side effects, and over the subsequent weeks and months the dosage is gradually reduced until the lowest efficacious dose is attained which will control the condition. A low dosage of the drug treatment is administered for several months or years in order to maintain the condition. It is important to be aware of the risk of infection to the skin, especially when blisters are broken. An antibacterial ointment is routinely applied to the skin for this purpose. In between flares, although the majority of people experience no outward evidence of the disease, it is advisable to keep the skin well hydrated using emollients (creams, lotions and bath oils). Some people find bathing with a non-scented oil very soothing, whilst others have reported an intolerance to any bathing. Some people report adverse reactions to strong sunlight. Although exposure to ultraviolet (UV) light has not been proven to precipitate or to exacerbate the condition, exposing the skin to strong sunlight is inadvisable as the use of steroid creams will have thinned the skin, thereby increasing the risk of skin damage due to sun exposure.
For further information contact:
Bullous Pemphigoid Support Group, 17 Barley Mount, Redhills, Exeter, EX4 1RP. The Bullous Pemphigoid Support Group aims to:
- offer support to people with bullous pemphigoid.
- establish commonality between experiences, in order to gain a greater understanding of the causes of the disease and treatment regimens.
DARIER'S DISEASE
This disease was first described in 1889 by Jean Darier, a French dermatologist. It is a rare condition characterised by itchy, warty bumps often involving the chest, neck and upper back. The condition can affect both men and women.
Symptoms
The first signs of the condition usually appear between the ages of 6 and 20, but may begin when people are older or, rarely, younger. The severity of the condition varies enormously and is unpredictable. Small brownish, rough topped bumps develop on the skin. Some patients have scattered spots which cause very little trouble, but in others the disease is more pronounced. The chest, neck or upper back are often involved at the beginning, but warty bumps may occur on any part of the body. It is unusual for people to have much trouble on the face, except for the skin on the forehead near the hairline. The scalp and skin around the ears may be scaly and itchy and most people notice some small spots in the armpits, the groin or, in women, under the breasts.
The fingernails are usually affected. They tend to be rather fragile, split easily and look as if they have been bitten or appear dirty. There may be very obvious long red or white lines running the length of the nails. Nail changes or flat warts on the backs of the hands are often present in childhood, before other symptoms appear. Pits or small corns occur on the palms of the hands and less often the soles of the feet. Occasionally there may be small spots inside the mouth, which give the roof of the mouth a rough feeling.
Although the condition is not infectious or contagious, people with disease show an increased susceptibility to herpes simplex infections, which exacerbates the symptoms of the condition. Though the skin may be clean, affected areas may smell unpleasant, due to bacterial growth in the rash. The condition is aggravated in the summer months due to an inherent photosensitivity, and through stress.
Causes
It is a dominantly inherited condition. There is a 1-in-2 chance that each child of an affected parent will inherit the disease.
http://www.intutionspasalon.com
http://www.ultimatespasalon.com
The condition is caused by a change (mutation) in a gene on chromosome 12. This gene makes a protein found within keratinocytes called SERCA2. The SERCA2 protein acts as
Cells use calcium to produce signals that control the complicated disease we believe signalling is faulty in the skin because the calcium pumps do not work properly. This leads to breakdown in the normal bonding of skin cells. The skin becomes scaly, lumpy and may blister.
Treatments
Retinoids (Vitamin A derivatives) are taken orally and improve the overall condition of the skin, by reducing its lumpiness and scaling, in most patients. Care must be exercised when prescribing to sexually active women, as retinoids could damage an unborn child. Therefore retinoids are only prescribed to sexually active women who have been sterilised, or who are using an effective contraceptive. Retinoids also cause the drying of lips, eyes and nose and patients with mild forms of the disease often decide to live with the symptoms of the condition rather than these side effects.
Itching (pruritus) is very common. Emollients containing an anti-pruritic may relieve some of the irritation. More severe pruritus can be controlled with a corticosteroid cream, containing an antibiotic to prevent skin infection. As mentioned the affected skin may smell unpleasant, particularly in moist areas, due to a bacterial growth in the rash. This does not mean that the skin is dirty. Careful washing is important, and antiseptic solutions for the bath, as well as creams or antibiotics may help.
The condition can be exacerbated by heat, sweating and, wool or nylon clothing. Some patients find that sunlight causes the skin to flare up, whilst some women find the condition worsens around the time of their period.
In a quarter of patients the condition improves as they get older. Most people lead full and active lives, with less than a quarter needing time off work or school because of the condition.
The Darier's Disease Support Group provides information and support to people with Darier's disease, with the motto
Please visit the fallowing site for skin care products:
Recommended Skin Care Store: www.intuitionspasalon.com
Cellex-C
Decleor
Dermalogica
Gatineau
Juvena
Md Formulations
Nelly De Vuyst
Sothys
SkinCeuticals
Physiodermie
Pupa Make up
Valmont
Yonka
www.skin-care.8k.com
www.acne.itgo.com
www.skin-care-renova.itgo.com
http://www.decleor-skin-care.itgo.com